Anti-Aging Senolytics Slow Bone Loss but Not Gum Disease
Study shows that dasatinib and quercetin reduce inflammation and prevent age-related alveolar bone loss in mice, supporting healthier aging gums.
Highlights
- Dasatinib and quercetin reduced age-related bone loss in mice, leading to smaller increases in tooth-to-bone distance and less root exposure over time.
- This senolytic treatment did not reduce bone loss in rats with periodontitis, a bacterial infection that drives rapid inflammation and tissue damage.
- The findings suggest that senolytic therapies may work best in conditions where senescent cells are a central driver of decline, rather than in fast-moving disease caused by infection.
Our bones depend on continuous remodeling to maintain their structure, and that process becomes less efficient with age. In the jaw, this appears as alveolar bone loss, where the bone supporting our teeth gradually recedes. This increases the distance between the tooth surface and surrounding bone and exposes more of the root, reducing structural support.
Researchers have increasingly focused on senescent cells as one contributor to this process. These cells persist in tissue and release signals that promote inflammation and tissue remodeling over time. In a study published in the Journal of Periodontology, Battistelli and colleagues tested whether removing these cells using a combination of dasatinib and quercetin could slow bone loss under two conditions: gradual aging and active disease.
Senolytics Reduce Age-Related Bone Loss
To determine whether senescent cells influence long-term bone decline, the researchers treated mice for over ten months starting in early adulthood. This design allowed them to observe how bone changes when senescent cells are periodically removed, rather than attempting to reverse existing damage.
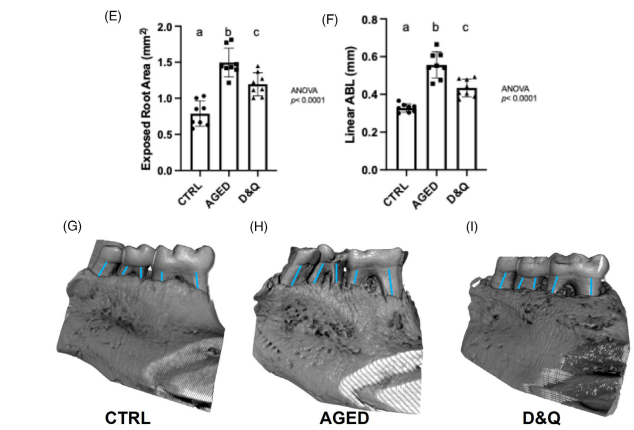
In untreated mice, aging led to a clear increase in the distance between the tooth and the bone crest (the top edge of the bone that surrounds and supports the tooth), along with a larger exposed root surface area (the portion of the tooth that becomes uncovered as bone recedes). In treated mice, both measurements still increased, but the increase was smaller. This means bone loss still occurred, but less bone was lost over the same period compared to untreated animals.
Senolytics Preserve Bone Across the Skeleton
To determine whether this effect was limited to the jaw, the researchers examined the strength of the femur, the largest bone in the body. In untreated aged mice, the outer layer of bone became thinner, and overall bone strength declined. In treated mice, these measurements remained higher, indicating that less structural loss occurred over time. This shows that removing senescent cells influences bones other than the jaw.
Senolytics Lower Inflammatory and Tissue Breakdown Signals
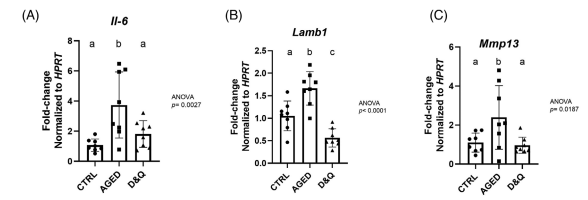
To understand the underlying biology, the researchers measured gene activity in alveolar bone, focusing on pathways involved in inflammation and tissue breakdown. In untreated aged mice, activity in genes such as Il6 (linked to inflammation), Mmp13 (involved in tissue breakdown), and Lamb1 (associated with structural tissue remodeling) was higher. In treated mice, activity in these genes was lower, indicating reduced inflammatory signaling and less degradation of structural tissue. These changes correspond with the smaller increases in bone loss observed in treated animals.
Senolytics Do Not Reduce Bone Loss in Gum Disease
The researchers then tested whether the same treatment could prevent bone loss during rapid disease. They induced periodontitis in rats, where a bacterial infection triggers inflammation and accelerates bone resorption (the breakdown and loss of bone tissue).
In this model, treated and untreated animals showed similar increases in bone crest distance and root exposure. These measurements indicate that the amount of bone lost was comparable between groups. The treatment did not reduce bone loss or slow its progression under these conditions.
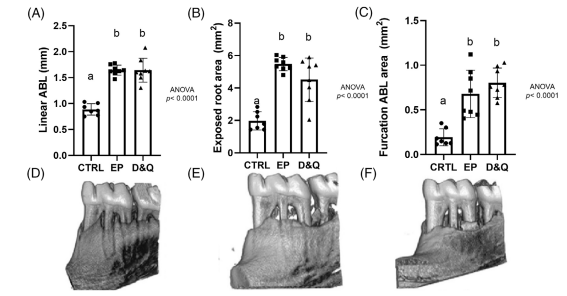
(Battistelli et al., 2026 | Journal of Periodontology) Senolytic treatment does not reduce bone loss in experimental periodontitis. Three-dimensional views of the jaw show bone structure in control (CTRL), experimental periodontitis (EP), and dasatinib plus quercetin-treated (D&Q) rats. Rats with gum disease show clear bone loss around the teeth, with more of the tooth root exposed. Treatment with dasatinib and quercetin does not reduce this bone loss, with treated animals showing a similar level of damage as untreated disease.
Timing and Dosing Determine Senolytic Effectiveness
When we compare the aging and disease models, the difference in treatment response comes down to how bone loss develops. In aging, structural decline occurs gradually, and preclinical studies suggest that senescent cells contribute directly to the process over time. Removing these cells reduces inflammatory signaling and limits the amount of bone lost across the treatment period.
In periodontitis, bone loss develops rapidly and is driven by bacterial infection and the immune response that follows. Much of the structural damage occurs early, before senolytic treatment can meaningfully alter the tissue environment. Because these therapies remove existing senescent cells but do not block the initial inflammatory response, the treatment does not reduce bone loss under these conditions.
These findings suggest that senolytics function most effectively as maintenance interventions that limit the accumulation of senescent cells before structural decline accelerates. Their effectiveness depends on timing, dosing frequency, and the rate at which damage develops in the tissue. Applying the same treatment strategy across conditions driven by different biological mechanisms can produce very different outcomes, which has direct implications for how these therapies are tested and used in clinical settings.
Dasatinib and Quercetin Reduce Senescent Cell Burden in Aging Models
Dasatinib and quercetin are among the most studied senolytic combinations. Dasatinib is an FDA-approved drug used to treat leukemia, where it inhibits signaling pathways involved in cell proliferation. Quercetin is a plant-derived flavonoid with anti-inflammatory and antioxidant properties that has been widely studied in metabolic and cardiovascular contexts.
Together, these compounds have been shown in multiple animal studies to selectively eliminate senescent cells and improve tissue function. In preclinical models, treatment with dasatinib and quercetin has been shown to reduce age-related bone loss and improve bone microarchitecture. Additional studies have linked this combination to improvements in survival and physical performance in aged mice.
Early human studies have also begun to translate these findings. In patients with diabetic kidney disease, intermittent dosing of dasatinib and quercetin reduced markers of senescent cell burden, providing initial evidence of senolytic activity in humans. Separate clinical work in idiopathic pulmonary fibrosis has shown improvements in physical function following short-term senolytic treatment.
Dasatinib can produce side effects at standard clinical doses, and its use in aging research relies on intermittent dosing strategies that aim to reduce senescent cell populations without disrupting normal tissue function. Quercetin has a more favorable safety profile, but its bioavailability varies depending on formulation. Current research focuses on optimizing dosing schedules that balance effectiveness with tolerability.
These findings suggest that dasatinib and quercetin may have the greatest impact when used early, before structural damage progresses beyond the point where removing senescent cells can meaningfully alter tissue outcomes.
Aging model: Male C57BL/6 mice aged 30 weeks at baseline and aged to 17.5 months during the study.
Dosage: Monthly oral gavage of dasatinib (5 mg/kg) plus quercetin (50 mg/kg) for 10 months.
 Comments
Comments