Creatine: A Potential Aid for Muscle Health in Alzheimer’s
Eight weeks of creatine monohydrate supplementation increases muscle strength and size in Alzheimer’s disease (AD) patients.
Highlights
- Creatine increases grip strength but not leg strength in AD patients.
- Creatine also increases thigh muscle size while reducing thigh fat in AD patients.
- Taking creatine could potentially contribute to the treatment of AD.
AD is a progressive neurodegenerative disorder that not only affects cognitive function but also often leads to a decline in physical capabilities, including muscle strength and mass. This physical decline can significantly impact the quality of life for individuals living with AD. Recent research has begun to explore interventions that may mitigate these effects, with creatine emerging as a compound of interest due to its established role in muscle energy metabolism and growth.
A pilot study published in Frontiers in Nutrition investigated the potential muscular benefits of creatine supplementation in patients with AD. The objective was to determine if an eight-week regimen could lead to improvements in muscle strength and size.
Creatine Improves Muscle Strength and Size
To assess the effects of creatine, researchers at the University of Kansas conducted a single-arm trial. This means that all participants received the intervention, and their progress was measured against their own initial pre-creatine data. The study involved 20 individuals diagnosed with probable AD-dementia. Each participant received 20 grams of creatine monohydrate daily for a period of eight weeks.
Strength
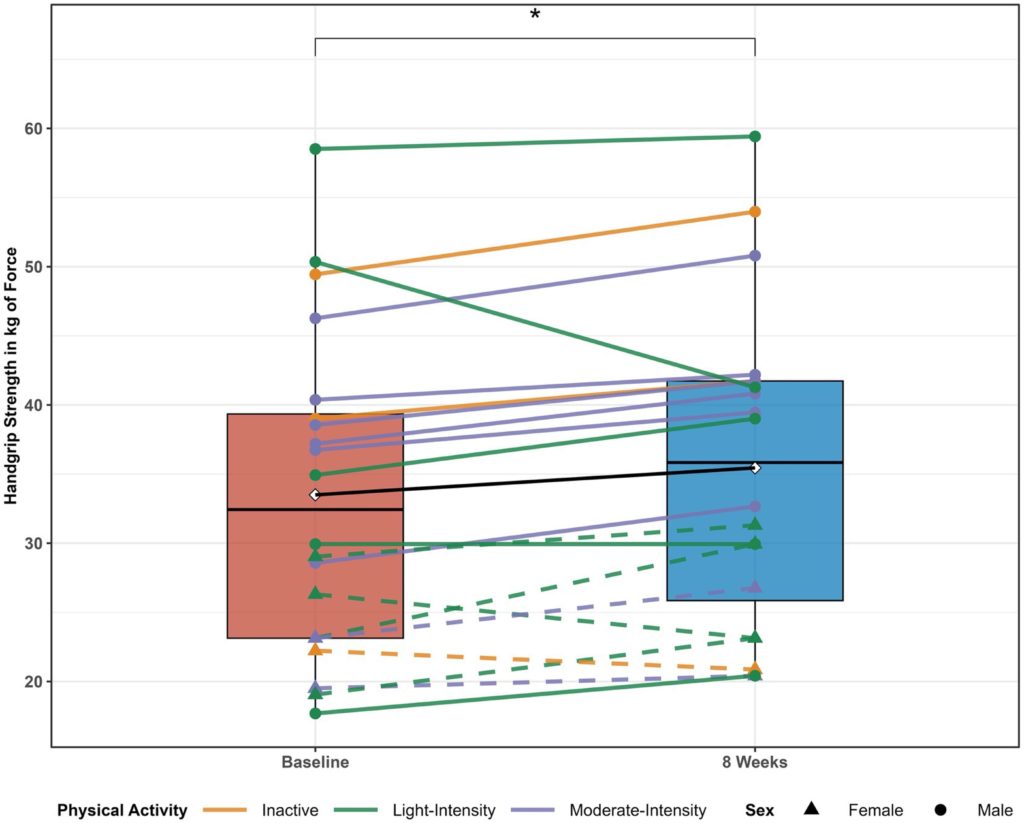
Several key metrics were used to evaluate changes in muscle health, including muscle strength. The participants showed a significant increase in handgrip strength, improving from their initial measurements by an average of 1.9 kilograms (4.2 pounds) of force. Handgrip strength is associated with a better quality of life and reduced mortality risk. Moreover, a subset of ten participants also underwent a lower-body strength assessment. However, there were no changes observed in leg strength. These findings show that creatine improves grip strength in AD patients.
Size
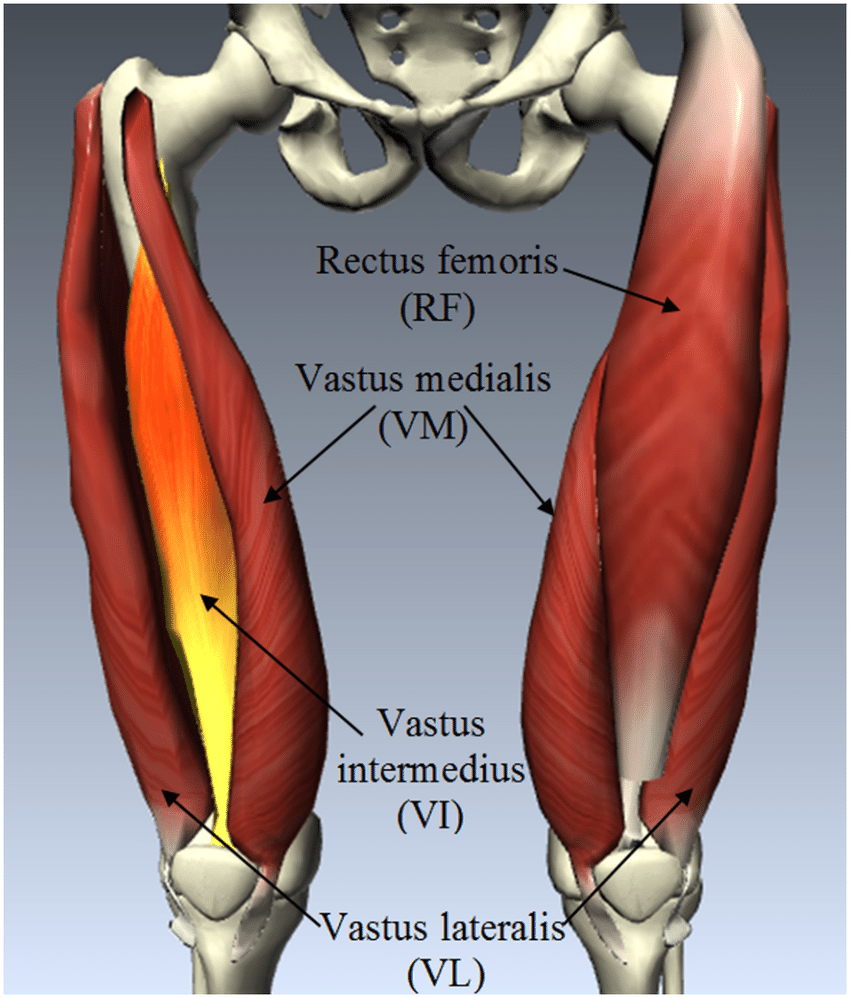
Muscle size was assessed using ultrasound imaging to measure the cross-sectional area of specific thigh muscles (rectus femoris, vastus medialis, and vastus lateralis) in 18 participants. Ultrasound provides a non-invasive way to visualize and quantify muscle dimensions. The cross-sectional area of two key thigh muscles, the rectus femoris and vastus medialis, significantly increased, indicating an increase in size. Moreover, subcutaneous fat decreased in the rectus femoris and vastus lateralis regions, suggesting improvements in body composition. However, there were no changes in overall body composition.
Limitations
Aside from the common limitations of a pilot study (small number of participants and no placebo group), one limitation arises from studies showing that creatine increases muscle size through water retention. Considering that an increase in leg strength was not observed, it is possible that the increase in leg muscle size exhibited by the participants was due to water retention. Moreover, the increase in grip strength could be due to improved neural and motor system capacity. Studies that control for muscle hydration levels may elucidate whether creatine increases muscle size in the absence of exercise in AD patients.
Can Taking Creatine Prevent Alzheimer’s Disease?
Since creatine has been shown in many studies to increase muscle strength and size, particularly in response to resistance training, it seems likely that AD patients would be affected similarly. However, in this study, resistance training was not part of the protocol. With that being said, future studies that combine creatine monohydrate supplementation with resistance training may lead to more robust results.
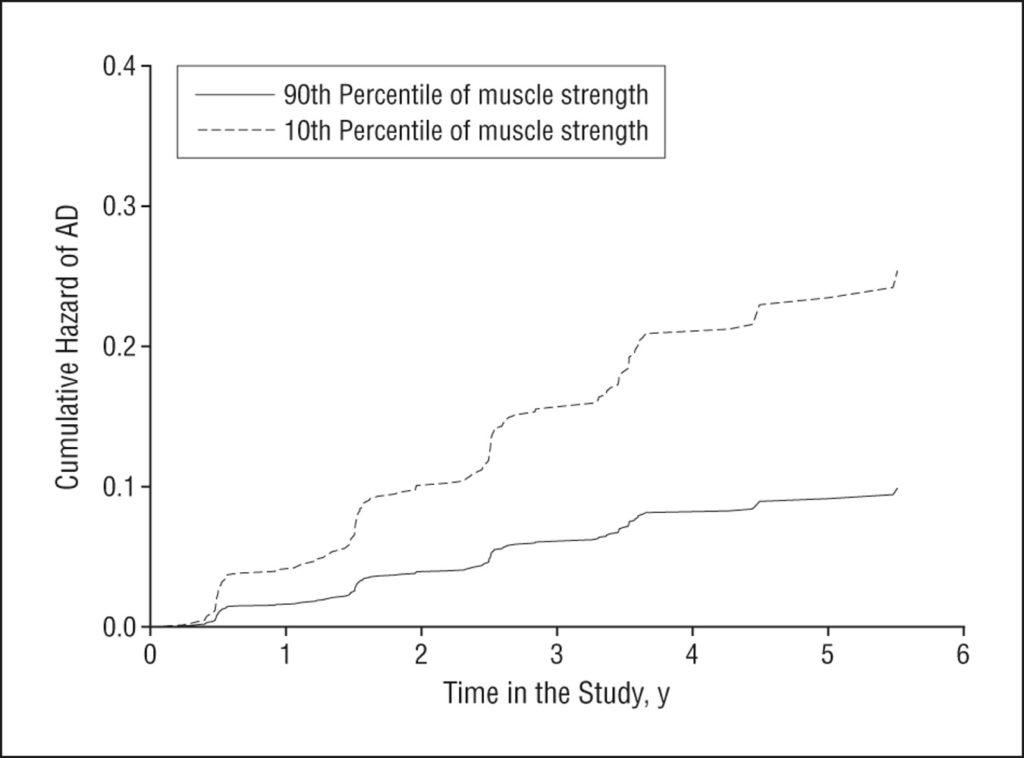
Assuming that, when combined with resistance training, creatine supplementation increases muscle strength, it is possible that creatine could prevent AD. This is based on a Rush University study showing that increased muscle strength is associated with a lower risk of AD. In the study, Rush researchers generated a muscle strength score based on strength measurements from 11 muscle groups. They found that for each increase in muscle strength score, there was a 43% decrease in the risk of AD.
Furthermore, in a previous study from the same University of Kansas researchers, it was shown that creatine supplementation improves the memory of AD patients. Additionally, a meta-analysis of 10 randomized controlled trials showed that creatine improves the memory of healthy adults. These findings suggest that creatine can improve brain function and potentially deter neurodegeneration and dementia. Nevertheless, the doses associated with these studies are much larger than 5 grams (the recommended dose for muscle hypertrophy), being closer to 20 grams.
Therefore, it may be possible that supplementing with about 20 grams of creatine monohydrate could assist in the treatment of AD. Due to its mysterious etiology, AD lacks effective treatments, yet many studies have shown that dysregulated energy metabolism is involved in its development. Namely, reduced glucose uptake and mitochondrial dysfunction contribute to lower levels of cellular energy currency, ATP. Creatine may be helpful in this respect, as it contributes to replenishing ATP levels faster.
Participants: Alzheimer’s patients
Dosage: 20 g of creatine monohydrate for eight weeks
 Comments
Comments