Peter Attia on Prolonging Life: Should You Take Statins Without Having Symptoms?
Taking cholesterol-lowering drugs like statins can reduce the risk of heart disease, thereby potentially reducing the risk of heart disease-related mortality.
Highlights:
- In a recent study, heart disease was observed in one-third of asymptomatic individuals, which was associated with LDL cholesterol levels.
- Dr. Attia alludes to taking LDL cholesterol-lowering drugs to mitigate the risk of heart disease.
- While statins can lower LDL levels, so can diet and exercise.
Heart disease is the number one leading cause of death in the United States with atherosclerosis — artery plaque buildup — being the primary suspect. As such, longevity specialist Peter Attia, MD, alludes to taking prescription medications, such as statins, to reduce the risk of atherosclerosis even if not experiencing symptoms.
Atherosclerosis in Asymptomatic U.S. Adults
In a recent article, Dr. Peter Attia reviewed a study by Faridi et al. showing that seemingly healthy individuals can have plaque in their arteries. The study included 40- to 65-year-olds who did not have traditional risk factors for atherosclerosis, including:
- Hypertension
- Diabetes
- Tobacco use
Despite including only “low-risk” individuals, Faridi et al. observed coronary artery plaques in 36% of participants. This was done using computed tomography (CT) angiography, a state-of-the-art X-ray imaging technique that can detect fine details within blood vessels, including artery plaques. Using a similar CT technique, Faridi et al. also observed that 25% of the participants exhibited early-stage artery calcification, a more advanced stage of plaque buildup. The findings reveal that over one-third of individuals may have plaque in their arteries without knowing.
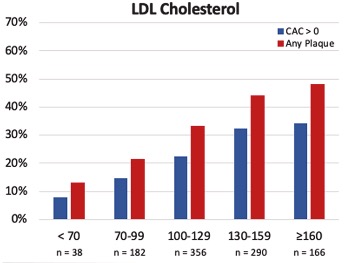
Furthermore, Faridi et al. took blood LDL cholesterol measurements from the participants and correlated them with artery plaque incidence. LDL cholesterol levels are given in mg/dL and below 100 mg/dL is considered optimal in adults without a history of atherosclerosis. However, artery plaques were detected in individuals with LDL cholesterol levels below 70 mg/dL, which is the recommended level among those with a history of atherosclerosis. Moreover, the researchers found that every 10 mg/dL increase in serum LDL cholesterol was associated with a 13% increased risk of artery plaques. These findings confirm the association between LDL cholesterol and atherosclerosis, but in “low-risk” individuals.
Faridi et al. also analyzed a subgroup of even healthier individuals by excluding participants who were overweight or obese and/or exhibited relatively high blood pressure values. Specifically:
- A systolic blood pressure <120 mm Hg and diastolic blood pressure <80 mm Hg
- A body mass index (BMI) <25 kg/m2
Within this subgroup, consisting of 84% women, 21% of individuals had coronary artery plaques and 15% exhibited early-stage plaque calcification. These findings further reveal that about one-fifth of individuals with relatively low blood pressure and healthy BMI have artery plaques without knowing.
Dr. Attia explains that this study points to millions of individuals in the United States unaware of having atherosclerosis because they suffer no symptoms, like shortness of breath or chest pain. As such, both patients and physicians may overlook the likelihood of atherosclerosis in seemingly healthy individuals, even when they have high LDL cholesterol levels.
Taking Statins to Lower Risk of Death
Atherosclerosis can lead to lethal cardiovascular events such as heart attacks or strokes. Dr. Attia says,
“[Atherosclerosis] is caused by apoB-containing lipoproteins (90-95% of which are low-density lipoproteins, or LDLs), which penetrate artery walls and initiate atherogenesis. Thus, therapies for lowering circulating LDL levels – such as statins, PCSK9 inhibitors, and others – have the power to virtually stop atherosclerosis in its tracks.”
It follows that LDL cholesterol-lowering drugs can potentially prevent or delay atherosclerosis-related events, which may contribute to prolonged lifespan in some individuals. Furthermore, Dr. Attia implies that since Faridi et al. showed that seemingly healthy individuals, as young as 40, can have artery plaques, it may be worth taking these drugs without having symptoms.
Study Limitations and Is Dr. Attia Right?
Faridi et al. did not have data on the dietary patterns and physical activity levels of the participants involved in their analysis. This poses two major limitations, considering that healthy dietary patterns and exercise reduce the risk of atherosclerosis. Structured aerobic and resistance exercise can reduce the risk of atherosclerosis by up to 50%. Thus, it is possible that the participants in the study who engaged in exercise and ate a healthy diet had the lowest LDL cholesterol, apoB, and artery plaques.
When it comes to cardiovascular disease (CVD)-related mortality, a diet consisting of higher amounts of fruits, vegetables, nuts, legumes, fish, and whole-fat dairy is associated with lower CVD and mortality in all regions of the world. Additionally, increased physical activity is strongly associated with lower CVD-related death. Therefore, eating a healthy diet and engaging in consistent exercise can prolong one’s lifespan. Whether combining LDL-lowering drugs with exercise is beneficial remains to be seen, as drugs such as statins may hinder exercise performance.
Dr. Attia may be right in cases where an individual exhibits high LDL cholesterol or apoB levels despite attempting to eat healthier and exercise. In cases where diet and exercise seem not to work, LDL-lowering drugs may be beneficial. LDL-lowering drugs may also be beneficial for those who are unable to consume a healthy diet and regularly exercise.
 Comments
Comments